
Mount Elizabeth Novena Hospital #10-48/49


WHAT IS AN
ANAL FISTULA?
An anal fistula is a small channel that can develop between the anal canal and the skin near the anus. They can occur if the abscess does not heal properly after the pus has drained away. It is estimated that between one in every four people with an anal abscess will develop a fistula. Less common causes of anal fistulas include Tuberculosis or Crohn’s disease (a long-term condition in which the digestive system becomes inflamed).
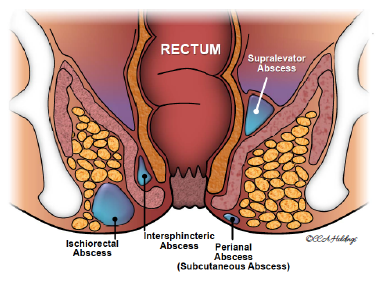
WHAT IS AN ANAL ABSCESS?
An anal abscess is a painful condition in which a collection of pus develops near the anus. An anal abscess is believed to originate from the anal glands, which are located between the internal and external anal sphincter and drain into the anal canal.
If the outlet of these glands becomes blocked, an abscess can form which can eventually extend to the skin surface. This often appears as a painful boil-like swelling near the anus.
WHAT ARE THE SYMPTOMS OF AN ABSCESS?
Superficial anal abscesses are often associated with:
- Painful swelling which worsens overtime when left untreated
- Skin irritation around the anus, including swelling, redness, and tenderness
- Discharge of pus
WHAT ARE THE SYMPTOMS OF A FISTULA?
Patients with fistulas commonly have a history of a previously drained anal abscess. Symptoms include:
- Anorectal pain
- Drainage from the perianal skin
- Irritation of the perianal skin
- Per Rectal bleeding
HOW IS AN ABSCESS TREATED?
Minor surgery may be performed to treat the abscess. Local anaesthesia or IV sedation may be used on the patient before an incision over the abscess is made. This opening enables pus to be drained from the infected cavity. After surgery, pain medications and antibiotics will be prescribed.
LOW VS. HIGH ANAL FISTULA
Low Fistula
The internal opening of the fistula begins below the puborectalis. The track passes through few or no sphincter muscle fibres and is close to the skin e.g. superficial fistulas, low intersphincteric fistulas, and low transsphincteric fistulas.
Low fistulas are easy to manage in the absence of complications and pose little threat to continence.
High Fistula
The internal opening of the fistula begins above the puborectalis. The track passes through or above a large amount of muscle; its route is more complicated and further away from the skin. e.g. high intersphincteric fistulas, high trans-sphincteric fistulas, suprasphincteric fistulas, and extrasphincteric fistulas.
Management of a high fistula is more complex than that of a low fistula.
A) Extrasphincteric Fistula
occurs outside the external anal sphincter and penetrates the levator muscle into the rectum
B) Transphincteric Fistula
crosses both the external and internal anal sphincter
C) Submucous Fistula
tracks beneath the internal and external anal sphincters
D) Intersphincteric Fistula
tracks between the internal and external anal sphincter muscles in the intersphincteric space
E) Suprasphincteric Fistula
travels outside the internal and external sphincters over the top of the puborectalis muscle and penetrates the levator muscle before tracking down to the skin

HOW IS A LOW FISTULA TREATED?
Fistulotomy
involves cutting along the whole length of the fistula to open it up so it heals as a flat scar.It is the most effective treatment for many anal fistulas. However, as the fistula often courses through the anal muscles, this method would require cutting through a portion of the sphincter muscles which could result in incontinence. Hence, ultrasonography is used to mark the location of the fistula. If the fistula is too high, more muscle would need to be cut. In order to preserve the muscle, other procedures below may be recommended instead.
HOW IS A HIGH FISTULA TREATED?
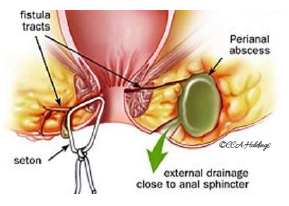
Seton Technique
involves a piece of surgical thread that is left in the fistula for several weeks to keep it open. This allows it to drain and helps it heal. To cure a fistula, tighter setons may be used to cut through the fistula slowly.
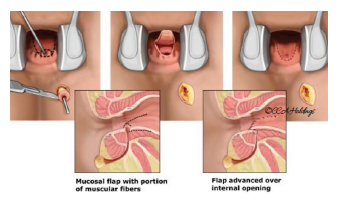
Advancement Flap Procedure
may be considered if your fistula passes through the anal sphincter muscles and if undergoing a fistulotomy puts you at high risk of incontinence.This involves cutting or scraping out the fistula and covering the original opening with a flap of tissue taken from inside the rectum.
Although its 85% success rate is lower than that of a fistulotomy, this procedure avoids the need to cut the anal sphincter muscles.
Ligation of the Intersphincteric Fistula Tract (LIFT)
procedure is designed as a treatment for fistulas that pass through the anal sphincter muscles, in which case a fistulotomy would be too risky.LIFT procedure is based on the secure closure of the internal opening and removal of infected cryptoglandular tissue through the intersphincteric approach. Essential steps of the procedure include: incision at the intersphincteric groove, identification of the intersphincteric tract, ligation of intersphincteric tract close to the internal opening and removal of intersphincteric tract, scraping out all granulation tissue in the rest of the fistulous tract, and suturing of the defect at the external sphincter muscle.
Ligation of intersphincteric tract
Anal Fistula Plug
is a minimally invasive and sphincter-preserving alternative to traditional fistula surgery. It is made from complex collagen obtained from animals. The plug is a conical device that is placed by being drawn through the fistula tract and suturing it in place.Once implanted, the plug incorporates naturally over time into the human tissue (human cells and tissues will ‘grow’ into the plug), thus facilitating the closure of the fistula.
*It is generally less effective than fistulotomy and the results may not be long-lasting
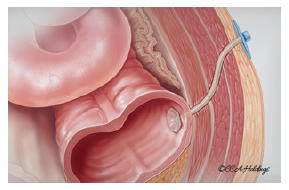
Fistula Plug is applied to help seal the fistula
SHOULD YOU UNDERGO ANAL FISTULA SURGERY?
Severity of Symptoms
If you're experiencing persistent pain, discomfort, drainage of pus or blood, recurrent infections, or other bothersome symptoms associated with your anal fistula, surgery may be recommended to alleviate these issues and improve your quality of life.
Location and Complexity of the Fistula
The location and complexity of the anal fistula play a crucial role in determining the appropriate treatment approach. Fistulas that are superficial and simple may respond well to non-surgical treatments, while complex fistulas that involve multiple tracts or are located in challenging anatomical areas may require surgical intervention for effective management.
Risk of Complications
Untreated or poorly managed anal fistulas can lead to complications such as abscess formation, recurrent infections, faecal incontinence, and anal stenosis. Surgery aims to eliminate the fistula tract and reduce the risk of complications associated with ongoing infection and inflammation.
Impact on Daily Life
Anal fistulas can significantly impact daily activities, including sitting, walking, and bowel movements, due to pain and discomfort. If your anal fistula is affecting your ability to perform routine tasks or impacting your overall well-being, surgery may be necessary to address the underlying problem and improve your quality of life..
Failure of Conservative Treatments
If conservative treatments such as antibiotics, analgesics, sitz baths, and dietary modifications have been unsuccessful in resolving your anal fistula or if the fistula recurs despite treatment, surgery may be recommended as a more definitive solution.
Health Status and Medical History
Your overall health status and medical history will also influence the decision-making process. Your healthcare provider will consider factors such as underlying medical conditions, surgical risks, and potential postoperative complications when determining the suitability of surgery for your specific case.
WHAT IS THE COST OF ANAL FISTULA SURGERY IN SINGAPORE?
The price of anal fistula surgery in Singapore can vary depending on several factors, including the specific type of surgery performed, the complexity of the anal fistula, the healthcare facility where the procedure is performed, the surgeon's expertise, and any additional services or amenities included in the treatment package.
You should speak to your doctor and get an estimate based on your condition and health needs.
HOW LONG DOES IT TAKE BEFORE PATIENTS FEEL BETTER?
Discomfort after fistula surgery can range from mild to moderate for the first week and can be managed with the use of painkillers.
WHAT ARE THE CHANCES OF RECURRENCE OF AN ABSCESS OR FISTULA?
Despite proper treatment and apparent complete healing, fistulas can potentially recur, with recurrence rates dependent upon the particular surgical technique utilized. Should symptoms suggesting recurrence arise, it is recommended that you find a colorectal surgeon to re-assess and manage your condition.
CONTACT YOUR DOCTOR IMMEDIATELY IF YOU:
Contact your doctor immediately if you:
- Notice rectal bleeding
- Have severe abdominal pain
- Develop a fever
- Feel very dizzy
- Experience vomiting
- Experience abdominal distention